
Report on the Highly Prevalent Health Issues in Tairawhiti
Student Name
School Name
健康问题代写 The major goal of this report is to explain the health issues in New Zealand in terms of the healthy behaviors and risk factors.
Executive Summary
Health issues have gained prominence in New Zealand by being the second sector to receive the largest share of the public financing. The government focus is to build an environment where better health behavior and care thrive. Good health creates a serene environment for economic prosperity where the government is able to focus the efforts on the economic activities.
The major goal of this report is to explain the health issues in New Zealand in terms of the healthy behaviors and risk factors. In this regard, this report will narrow down to study Tairawhiti region and review health issues that affect its population. Various literature will be referred in support of statistical analysis used and various research made over the years.
This report covers but not limited to the following areas of interests:
- The detailed demographic aspects of Tairawhiti and the analysis of its population.
- Health issues affecting Tairawhiti including illicit drugs, physical exercise, body weight and tobacco use.
Table of Contents 健康问题代写
Table of Contents
Executive Summary —————————————– 2
Table of Contents —————————————– 3
Introduction —————————————– 4
About Tairawhiti —————————————– 4
Health Issues in Tairawhiti —————————————– 5
Tobacco Use —————————————– 6
Tairawhiti Prevalence to Smoking Use —————————————– 6
Illicit Drug Use – Amphetamine —————————————– 8
Amphetamine use in Tairawhiti —————————————– 9
Physical Exercise —————————————– 10
Little or no Physical Exercise in Tairawhiti —————————————– 11
Body Size —————————————– 12
Over-weight and Obesity in Tairawhiti —————————————– 13
References —————————————– 16
Appendices —————————————– 17
Introduction 健康问题代写
This report explores the health issues in New Zealand in terms of health behaviors and risk factors. Health behaviors and risk factors contribute may contribute to health problems and diseases. The health issues addressed in this report include:
- Prevalences on tobacco use in different levels of age in New Zealand.
- Illicit drug use where prevalences to the use of amphetamine in different age groups will be analyzed.
- The physical exercise which will narrow down to people prevalent little or no physical exercise.
- Body size – the report will provide statistical representation on prevalences of different cohorts on unhealthy living with overweight and obesity.
About Tairawhiti 健康问题代写
This report chooses Tairawhiti region as the main area of interest to study the health issues affecting people of New Zealand. Tairawhiti is one of the highly deprived areas in New Zealand with a deprivation index of 7.
The Tairawhiti region is most eastern district and one of the most remote regions of New Zealand with a land area of roughly 3% of the country and the population of 1% of the whole New Zealand (Hauora Tairawhiti). The region has a population density of 5.6 per km square. The region is predominantly mountainous and ruggedness of the land. Gisborne City is the main urban center.
According to Census (2013), Tairawhiti region has the most diverse population when compared with other regions in New Zealand. The census highlighted that:
- The population of Tairawhiti is 43,656 which make approximately 1% of the population and is at position14thout of 16 regions by size in New Zealand.
- Maori residents are the largest in the region with a population of 19,683 forming 48.9% of the whole population.
- 48% of the local population of Tairawhiti is the youths below the age of 25 years with growing aging population.
The largest population of Tairawhiti lives outside the urban areas with large rural presenting various challenges in terms of access to the healthcare facilities. Following are the areas of interest with regard to the health condition of Tairawhiti:
- The region has a deprivation score of 7, where 1 and 10 represent the least deprived area and the most deprived area respectively.
Area deprivation
Distribution by NZDep 2013 decile, Tairāwhiti DHB, 2013
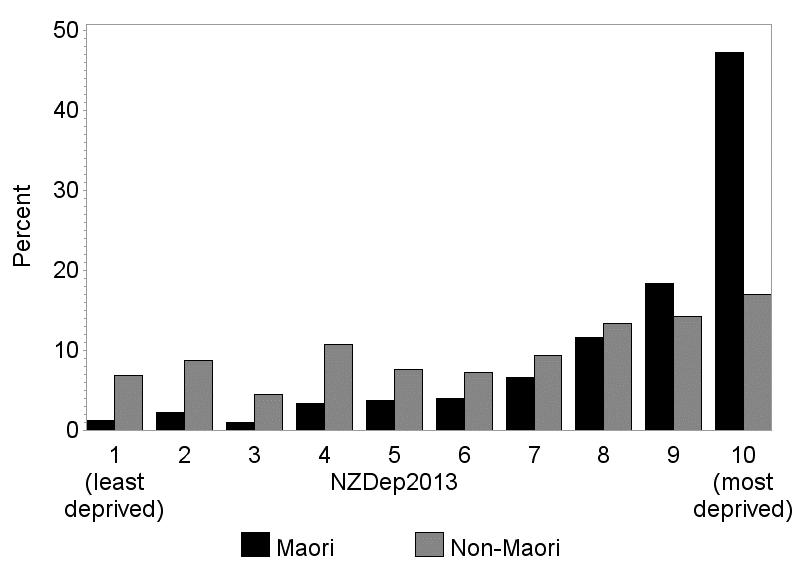
Source: 2013 Census, Statistics New Zealand. Atkinson J, Salmond C, Crampton P. 2014. NZDep2013 Index of Deprivation. The University of Otago Wellington.
- The deprivation score in Tairawhiti ranges from 2 in Wainui to 10 Ruatoria and Te Karaka.
- 52% of children between the ages of 0-14 are found in the most deprived area.
- The largest employment in Tairawhiti come from Health, Education, Agriculture, Horticulture, Forestry, and Fishing.
Health Issues in Tairawhiti
Being one of the deprived areas in New Zealand, Tairawhiti is faced with various health problems ranging from tobacco use, illicit drug abuse, body weight etc. citing various statistical evidence and research this essay will provide a detailed report on the above-mentioned health issues in Tairawhiti.
Tobacco Use
According to Tairawhiti District Health Board Annual Report, 2016/17 tobacco is ranked one of the leading causes of morbidity and premature mortality. It has also caused estimated death of 5,000 people in New Zealand every year and has been ranked as one of the major factors causing death in 2 out of 8 worldwide. Smoking s also considered the major contributor to preventable diseases and health conditions such as heart and respiratory disease and cancer. In addition, tobacco use has imposed an economic burden to individual smokers, families and the health system of Tairawhiti. Smokers spend significant money on buy tobacco which could have been directed to other life necessities such as nutrition, health, and education (Crengle et al, 2013).
According to Annual Data Explore 2016/17 of the Ministry of Health IN New Zealand establish that those currently smoking are:
- There was a drop in current smokers in 2016/17 with about 600,000 (15.7%) adult smokers down from 20.1% in 2006/07
- There was a drop in Maori Adult current smokers of 35% from 42% in 2006/07
- There are 24% Pacific adult current smokers without a significant drop from the previous survey.
- Smoking prevalence for young adults was reduced significantly but no significant decline in smoking by adults aged 35 years and above.
- Social-economic factors were a common determiner of the adult current smoking habits. It was found that most adults in social-economically deprived areas 3 times higher prevalence to be current smokers.
Tairawhiti Prevalence of Smoking Use 健康问题代写
Smoking tobacco in Tairawhiti has had a bad history for decades. There many efforts which have been established over the years to reduce the number of tobacco users in the region. As we will explore, their efforts have been effective.
In the New Zealand health survey of 2006-2007, it was established that Tairawhiti had the highest number of smokers of all district health boards. Out of the Tairawhiti population, over 30% were smokers which formed the highest smokers in the region. Tobacco use accounted for 70 deaths per year in Tairawhiti which more the deaths were Maori.
The following statistical data is according to the 2013 census statistics of New Zealand on the smoking prevalence in Tairawhiti region.
Smoking
Figure 2: Trends in the proportion of students aged 14–15 years who have never smoked, by gender, Tairāwhiti DHB, 1999–2013
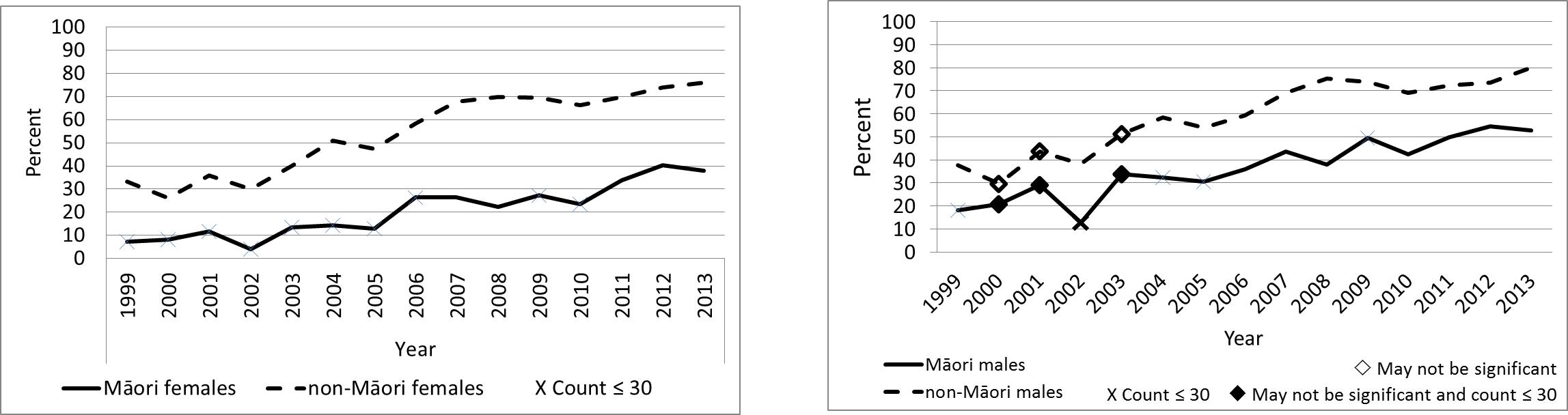
Source: ASH Year 10 Snapshot Survey, 2013
From the figure, over the last decade and a half Tairawhiti has had a significant increase in numbers of smokers. 49% had had never smoked in 2013.
Figure 3: Regular smokers, ages 15–17, 18–19, 20–24 years, Tairāwhiti DHB, 2013
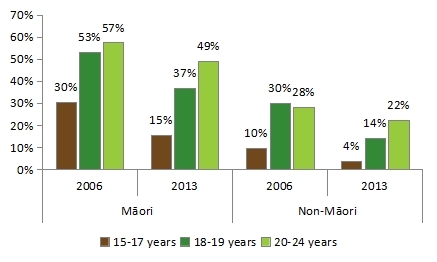
Source: 2013 Census, Statistics New Zealand
Note: Regular smokers smoke one or more cigarettes per day.
From the figure prevalence of smoking has significantly decreased in youths in Tairawhiti since 2006. However, among those aged 18-24 years have a higher prevalence of smoking in young adulthood. The 49% of Maori between the ages of 20-14 years were smoking regularly in 2013. On the other hand, Non-Maori were half as likely as Maori to smoke regularly in each group
Smoking status 健康问题代写
Table 38: Cigarette smoking status, 15 years and over, Tairāwhiti DHB, 2006 and 2013
| Smoking status | Māori | Non-Māori | Māori/non-Māori
ratio (95% CI) |
Difference in proportion | ||||||||
| Number | % | (95% CI) | Number | % | (95% CI) | |||||||
| 2006 | ||||||||||||
| Regular smoker | 5,265 | 45.2 | (44.3, | 46.1) | 3,363 | 23.3 | (22.5, | 24.1) | 1.94 | (1.87, | 2.02) | 21.9 |
| Ex-smoker | 2,256 | 17.0 | (16.4, | 17.7) | 4,242 | 19.4 | (18.7, | 20.1) | 0.88 | (0.83, | 0.92) | -2.4 |
| Never smoked | 4,554 | 37.7 | (36.8, | 38.6) | 9,414 | 57.2 | (56.3, | 58.1) | 0.66 | (0.64, | 0.68) | -19.5 |
| 2013 | ||||||||||||
| Regular smoker | 4,482 | 38.4 | (37.5, | 39.3) | 2,373 | 16.5 | (15.8, | 17.2) | 2.33 | (2.22, | 2.45) | 21.9 |
| Ex-smoker | 2,832 | 19.7 | (19.0, | 20.4) | 4,344 | 19.7 | (19.1, | 20.4) | 1.00 | (0.95, | 1.05) | 0.0 |
| Never smoked | 5,127 | 41.9 | (41.0, | 42.8) | 9,711 | 63.6 | (62.7, | 64.5) | 0.66 | (0.64, | 0.68) | -21.7 |
Source: 2006 and 2013 Censuses, Statistics New Zealand
Notes: % is age-standardized to the 2001 Māori population
Regular smokers smoke one or more cigarettes per day.
The statistics show a significant decline in the proportion of Maori adult regular smokers between 2006 and 2013 from 45% to 38%. The proportion of Maori non-smokers and ex-smokers has increased. However, a difference of 22% between Maori and Non-Maori smoking rates exist in Tairawhiti in 2013.
The current standing of the smokers according to the Annual Data Explorer 2014-2017 Publication of Ministry of Health New Zealand, places the Tairawhiti the leading in tobacco use in New Zealand.
Illicit Drug Use – Amphetamine 健康问题代写
According to the Amphetamine Use 2014/15: New Zealand Health Survey targeting the whole of New Zealand, 0.9% of adults used amphetamines in the past year. This equated to about 26,000 of the New Zealand population. The average past year use of the drug was 33 years up from 29 years in 2012/13.
The younger adults between ages 25-34 were more prevalent to have used amphetamines in the past year, followed by those aged 16-24 years. The lowest users of amphetamine were those aged 55-64 years.
However, the prevalence of the past-years amphetamine users aged 16-24 has been on decline trend since 2012-13. The statistics also show that past-year amphetamine use was higher among males at 1.2% than female at 0.7%.
The survey also established that Maori have a higher prevalence of using amphetamine than in-Maori. In the past year, 1.6% of Maori, 0.1% of Asians adults, 0.2% of Pacific adults, and 1.1 of European adults used amphetamine. Maori were found to be 1.8 times more prevalent in using amphetamine than non-Maori in the past year.
Table 1: Past-year amphetamine use in New Zealand for adults aged 16–64 years 健康问题代写
| Year | Survey | Mode | Prevalence |
| 2003 | Health Behaviours Survey – Drug Use | Telephone interview | 2.7% (2.3–3.3) |
| 2007/08 | New Zealand Alcohol and Drug Use Survey | Self-completed interview | 2.2% (1.7–2.7) |
| 2011/12 | New Zealand Health Survey | Face-to-face interview | 0.9% (0.7–1.1) |
| 2012/13 | New Zealand Health Survey | Face-to-face interview | 0.9% (0.7–1.2) |
| 2013/14 | New Zealand Health Survey | Face-to-face interview | 1.1% (0.8–1.4) |
| 2014/15 | New Zealand Health Survey | Face-to-face interview | 0.9% (0.7–1.1) |
Source: Ministry of Health 2007, Ministry of Health 2009; data from NZHS 2011/12, 2012/13, 2013/14 and 2014/15
Amphetamine use in Tairawhiti
According to the Annual Data Explorer 2014-2017, Tairawhiti stands at 0.8% (CI 0.2-2.0) prevalence for amphetamine use. The data show a significant increase in amphetamine use from 0.5% (CI 0.1-1.5) in 2011-14 to 0.8% (CI 0.2-2.0) in 2014-17 for adults aged 15 years and above.
Young adults aged 15-24 years have the highest prevalence in using amphetamine at 2% (CI 0.1-9.4). The population aged 45-64 years was least likely to use amphetamine at 0.2% (CI 0.0-1.1)
Generally, men aged 15-24 have a higher prevalence of 3.6% (CI 0.1-20.0) than women at the same age set, have the prevalence of 0.6% (CI 0.0-6.3). Maori women are more likely to use amphetamine at 1.2% (0.4-3.0) than their male counterpart at 0.4% (CI 0.0-2.7).
These charts give the prevalence in the specified population (that is, the percentage of the population affected)
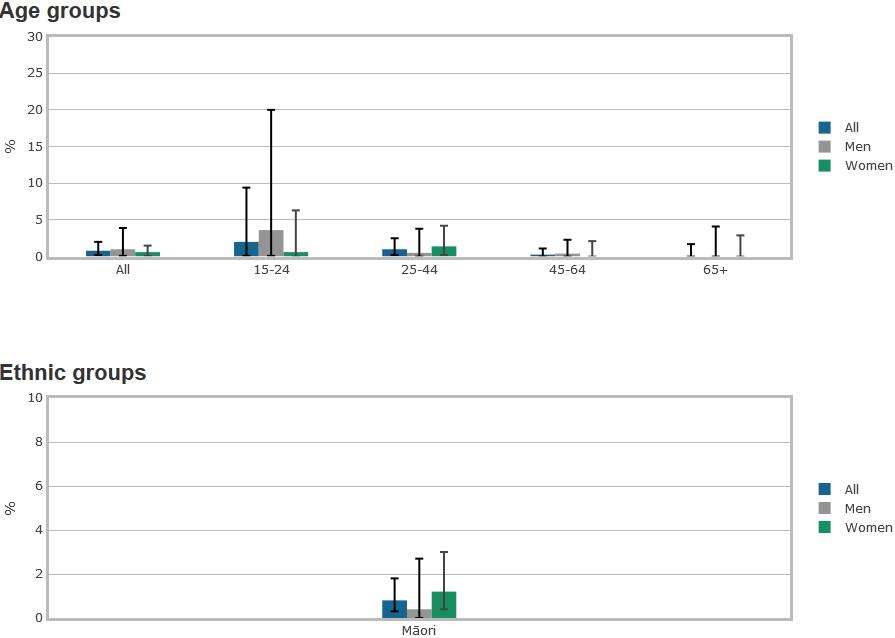
Source: Annual Data Explorer 2014-17
Physical Exercise 健康问题代写
New Zealand spends more than $ 13.2 billion dollars per year on health which account for 19% of the total annual expenditure (Ministry of Health 2011a). therefore it has become important for the government of New Zealand to promote preventative health care for its population to ensure a sustainable health care system.
Physical exercise is part of the activity which is used for preventive health care. Doing exercise regularly reduces risks of developing cardiovascular disease and general body health care. Daily physical activity for 30 minutes is crucial for health improvement.
Physical activity has the following importance to the health:
- Improving your cholesterol level
- Lowering your blood pressure
- Helping with weight loss and maintaining a healthy weight
- Controlling your blood glucose (sugar) level
- Helping you sleep better and feel less stressed
Little or no Physical Exercise in Tairawhiti
Generally, the population aged 65years and above has a higher prevalence of 38.1% (CI 29.8-47.2) for little or no physical exercise, compared with any other age group in Tairawhiti population. Women across all the age groups from 15 years and above have a higher prevalence of little or no physical exercise than men in the same age group. Maori women have the highest prevalence of 38.2% (CI 30.9-46.0) for lack of physical exercise.
These charts give the prevalence in the specified population (that is, the percentage of the population affected)
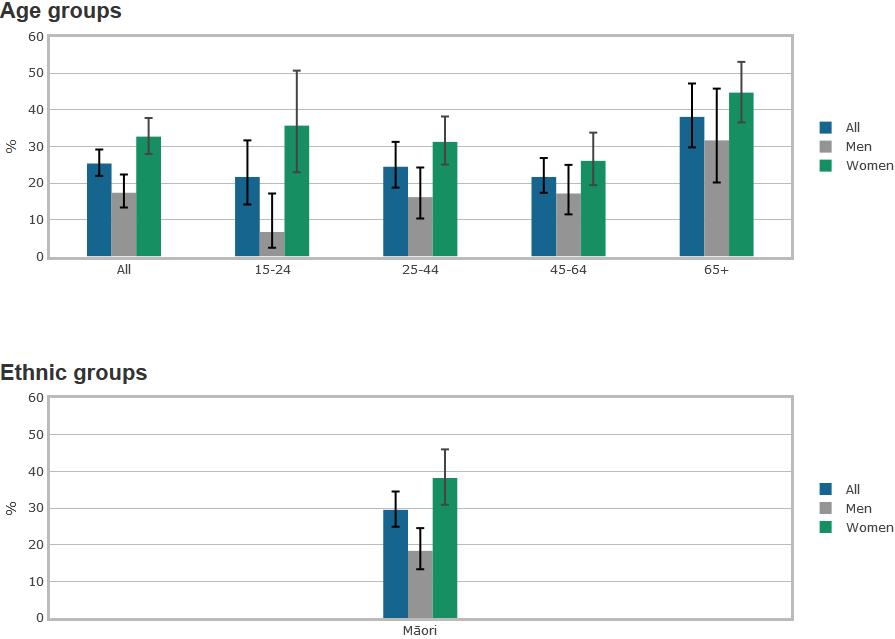
Source: Annual Data Explorer 2014-17
Body Size 健康问题代写
Under this subtopic, this report will explore the current status of the obesity epidemic in New Zealand. It will discuss the subgroups of the population that are affected most by the obesity on different age sets. It will also look at the most prevalent group of individuals in the population set.
Overweight is one of the risk factors for various diseases, including heart disease, stroke, type 2 diabetes and other types of cancer. Obesity also increases the risk of infertility, musculoskeletal problems, sleep apnoea and gout (WHO 2000). According to the Ministry of Health (2013a), high body mass index (BMI) is one of the top three risk factors contributing to ill health and disability in New Zealand. Life expectancy in obese people is shortened by approximately 8-9 years (Whitlock et al 2009).
OECD (2014), there has been a drastic increase in the global prevalence of obesity over the past decades. In New Zealand, obesity and over-weight has affected more than two-thirds of the adult population and a third of children. The prevalence of obesity in adults has increased in three folds from 10% in 1977 to 30% between 2011-13 in New Zealand.
Swinburn (2008), explained the reason for the increase in obesity, which is largely attributed to the modern lifestyles and living environment.
Reductions in physical exercise together with the presence of cheap, energy-dense and nutrient-poor foods have been witnessed in over the last three decades. This report looks at how obesity epidemic has impacted different birth cohorts in Tairawhiti.
Below is a summary of new Zealand obesity statistics. From the figure, between 2011-2013, it was found that 35% of New Zealand population adults were overweight and 30% were obese. Males have a high prevalence of 39% to be overweight than a female with 30%. Also, the obesity increased with age reaching optimum at 65-74 years.
Figure 1: Proportion of adults in each BMI category, 2011–2013
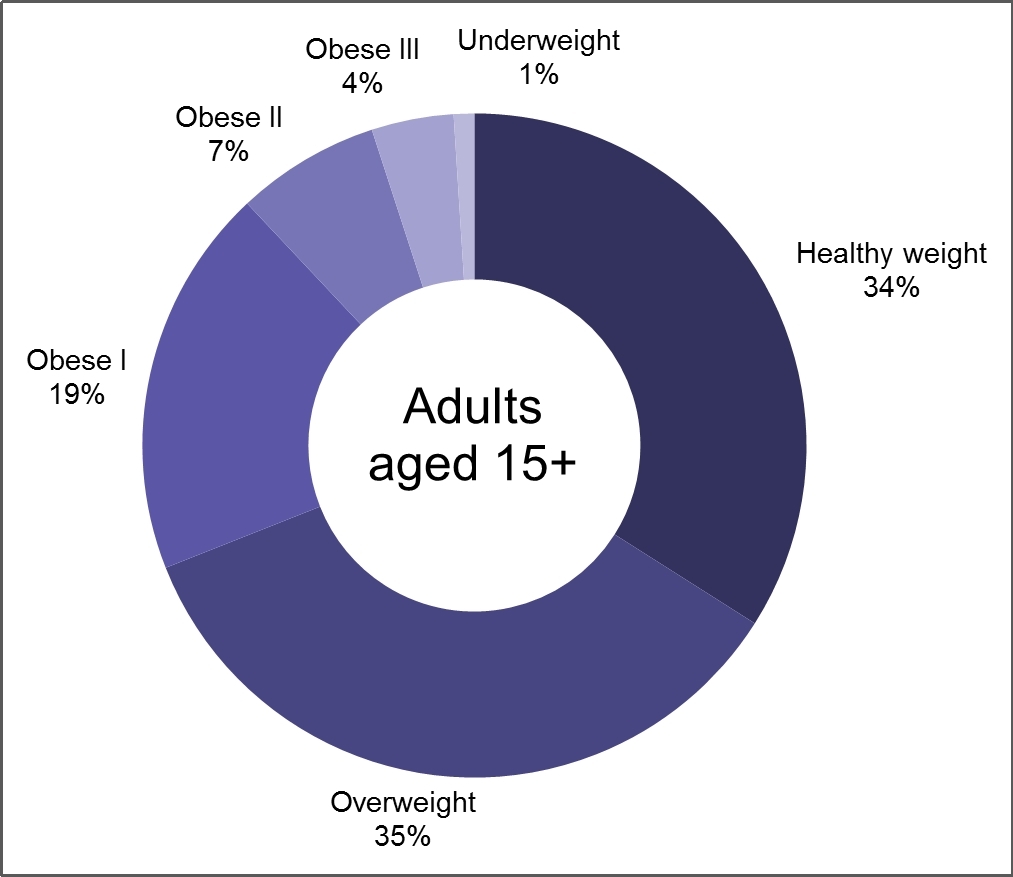
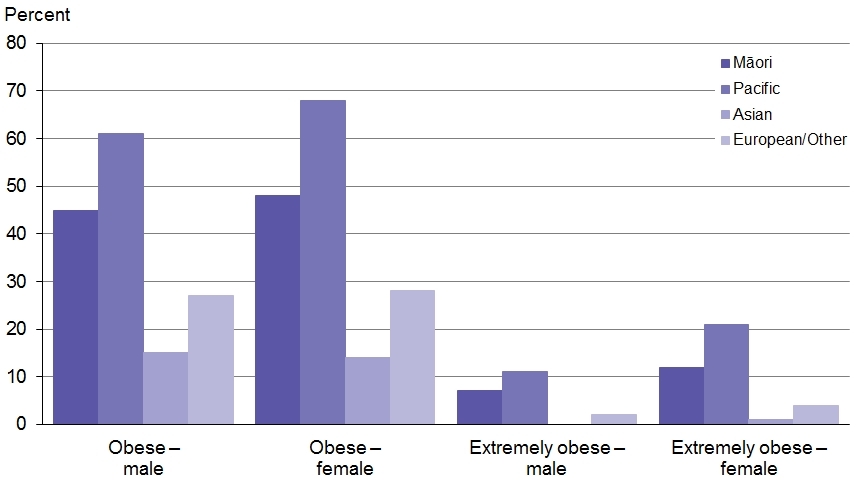
Figure 2: Rates of obesity and extreme obesity, by sex and ethnic group, 2011–2013
Over-weight and Obesity in Tairawhiti 健康问题代写
According to the Annual Data Explorer 2014-17, Tairawhiti is ranked 4th with 71.8% (CI 66.6-76.6) prevalence of overweight and obesity. There was an increase over-weight and obesity from 2011-2014 71.2% (CI 65.2-74.8) prevalence to 2014-2017 71.8% (CI 66.6-76.6) prevalence in Tairawhiti.
On average, there is a higher prevalence of overweight and obesity at the ages from 45 years and above. The prevalence levels increase with age with 45 years and above is the most deprived of prevalence level of more than 72%. Men have the higher prevalence of being overweight and obesity than women, averaging at more than 82% prevalence level.
These charts give the prevalence in the specified population (that is, the percentage of the population affected)
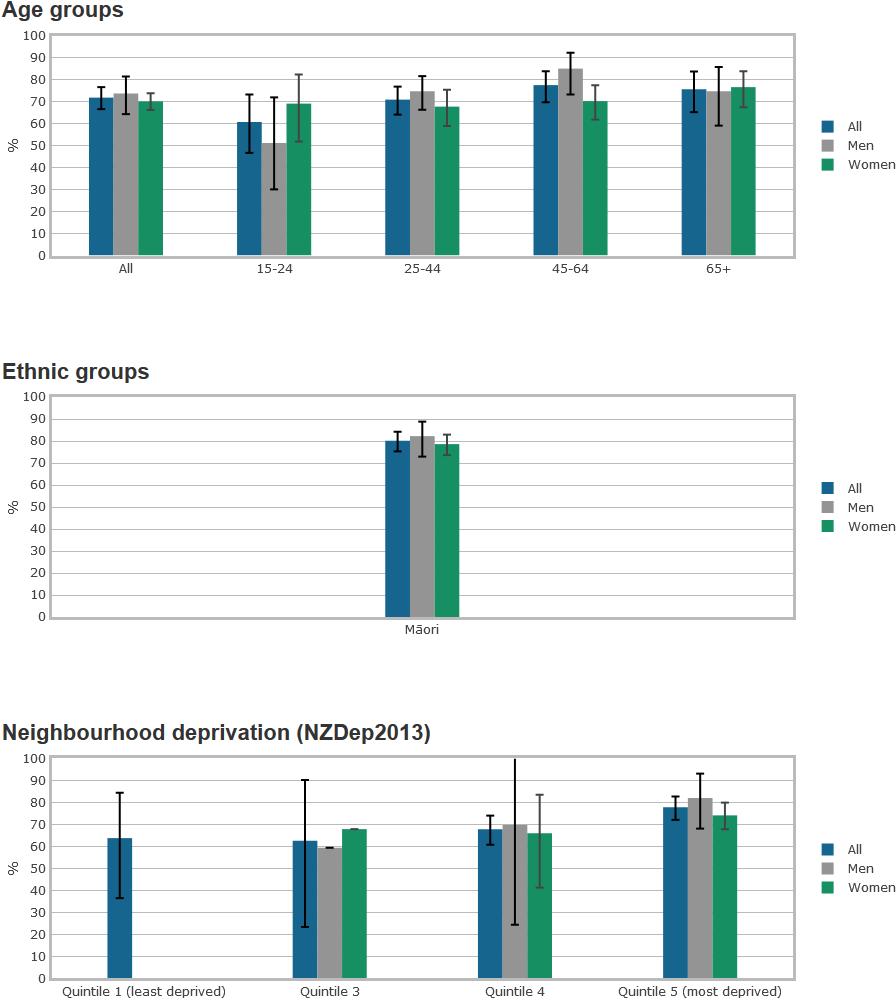
Source: Annual Data Explorer 2014-17
In the contemporary world, the healthy population has been the priority of the government and the society as a whole. Health issues that impact on the well-being of the people need to be addressed and sustainable solutions implemented. New Zealand is affected by the risk factors which has resulted in health problems to significant numbers in different age cohorts. On the other hand, health issues in Tairawhiti region, indicate high deprivation to the population. Many efforts have been put forth by both the community and the government of New Zealand to elevate population out of these risk factors.
References 健康问题代写
Annual Data Explorer. (2017, May 10). Regional Results 2014-2017: New Zealand Health Survey. Retrieved from https://www.health.govt.nz/publication/regional-results-2014-2017-new-zealand-health-survey
OECD. 2014. OECD Obesity Update 2014. Paris.
ASH Year 10 Snapshot. (2013). ASH Year 10 Snapshot smoking survey. Retrieved from https://www.hpa.org.nz/sites/default/files/documents/NZYTM%20information%20for%20people%20working%20with%20schools-FINAL.pdf
New Zealand Census. (2013, March 5). Census | Stats NZ. Retrieved from https://www.stats.govt.nz/topics/census
Ministry of Health. 2013a. Health Loss in New Zealand: A report from the New Zealand Burden of Diseases, Injuries and Risk Factors, 2006–16. Wellington: Ministry of Health.
Whitlock G, Lewington S, Sherliker P, et al. 2009. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet 373(9669): 1083–96.
Swinburn B. 2008. Obesity prevention: the role of policies, laws, and regulations. Australia and New Zealand Health Policy 5(1): 12.
Ministry of Health. 2007. Drug Use in New Zealand: Analysis of the 2003 New Zealand Health Behaviours Survey – Drug Use. Wellington: Ministry of Health.
WHO. 2000. Obesity: Preventing and managing the global epidemic. Report of a WHO Consultation (WHO Technical Report Series 894).
Hauora. (n.d.). Tairawhiti – region » Tairawhiti District Health. Retrieved from http://www.tdh.org.nz/about-us/tairawhiti-our-region/
Appendices
关于塔拉希提岛高度流行的健康问题的报告
学生姓名
学校名称
健康问题代写本报告的主要目的是从健康行为和危险因素的角度解释新西兰的健康问题。
执行摘要
在新西兰,卫生问题已成为第二个获得公共资金最多份额的部门,从而引起了人们的关注。政府的重点是营造一个环境,使健康的行为和护理得到更好的发展。良好的健康状况为经济繁荣创造了宁静的环境,使政府能够将精力集中在经济活动上。
本报告的主要目的是根据健康行为和危险因素来解释新西兰的健康问题。在这方面,本报告将缩小研究塔拉威提地区的范围,并审查影响其人口的健康问题。多年来将引用各种文献来支持所使用的统计分析和进行的各种研究。
本报告涵盖但不限于以下领域:
Tairawhiti的详细人口统计资料及其人口分析。
影响塔拉威提的健康问题,包括非法药物,体育锻炼,体重和烟草使用。
目录 健康问题代写
目录
执行摘要—————————————– 2
目录——————————————- 3
简介——————————————— 4
关于Tairawhiti 4
泰拉希提岛的健康问题——————————————————— 5
烟草使用—————————————– 6
Tairawhiti吸烟率——————————————— 6
非法药物使用-安非他明—————————————— 8
在塔拉希提岛使用苯丙胺—————————————– 9
体育锻炼——————————————- 10
泰拉希提岛很少或根本没有体育锻炼——————————————————— 11
身体尺寸——————————————- 12
Tairawhiti的超重和肥胖症——————————————————— 13
参考文献——————————————- 16
附录————————————————- 17
简介 健康问题代写
本报告从健康行为和危险因素的角度探讨了新西兰的健康问题。健康行为和危险因素可能导致健康问题和疾病。本报告涉及的健康问题包括:
新西兰不同年龄段的烟草使用流行率。
将分析不同年龄组苯丙胺使用率的非法药物使用情况。
体育锻炼将缩小到很少或根本没有体育锻炼的人们。
体型-该报告将提供有关不同人群超重和肥胖不健康人群患病率的统计数据。
关于Tairawhiti健康问题代写
本报告选择泰拉维希蒂地区为主要研究领域,以研究影响新西兰人民的健康问题。 Tairawhiti是新西兰的一个高度贫困的地区之一,贫困指数为7。
Tairawhiti地区是新西兰最东部的地区,也是新西兰最偏远的地区之一,土地面积约占新西兰的3%,人口占整个新西兰的1%(Hauora Tairawhiti)。该地区的人口密度为每平方公里5.6。该地区主要是山区和崎ness不平的土地。吉斯本市是主要的城市中心。
根据人口普查(2013年),与新西兰其他地区相比,塔拉威提地区的人口最多。人口普查强调:
Tairawhiti的人口为43,656,约占总人口的1%,在新西兰的16个地区中,其排名为第14位。
毛利人是该地区最大的居民,人口19,683,占总人口的48.9%。
Tairawhiti当地人口的48%是25岁以下的年轻人,这些年轻人的年龄在不断增长。
泰拉希提(Tarawhiti)人口最多,居住在城市地区以外,农村人口众多,在获得医疗保健设施方面面临各种挑战。以下是有关Tararawhiti的健康状况的关注领域:
该区域的剥夺得分为7,其中1和10分别代表剥夺最少的区域和剥夺最多的区域。
区域剥夺
NZDep 2013十分位数的分布,TairāwhitiDHB,2013年
资料来源:2013年人口普查,新西兰统计局。 Atkinson J,Salmond C,Crampton P.2014。NZDep2013贫困指数。奥塔哥大学惠灵顿分校。
Tairawhiti的剥夺评分从Wainui的2到Ruatoria和Te Karaka的10。
在最贫困的地区发现了52%的0-14岁儿童。
塔拉希提岛最大的就业机会是卫生,教育,农业,园艺,林业和渔业。
Tairawhiti的健康问题
作为新西兰的贫困地区之一,塔拉威提面临着各种健康问题,包括吸烟,非法药物滥用,体重等。根据各种统计证据和研究,本文将就上述健康问题提供详细的报告。在Tairawhiti。
烟草使用
根据Tairawhiti地区卫生局年度报告,2016/17烟草被列为发病率和过早死亡的主要原因之一。据估计,它每年在新西兰也造成5,000人死亡,在全世界8个国家中,有2个被认为是造成死亡的主要因素之一。吸烟也被认为是可预防疾病和健康状况的主要贡献者,例如心脏病和呼吸系统疾病以及癌症。此外,烟草使用给个人吸烟者,家庭和塔拉希提(Tarahhiti)的卫生系统带来了经济负担。吸烟者在购买烟草上花费了大量资金,这些钱本可以用于其他生活必需品,例如营养,健康和教育(Crengle等,2013)。
根据新西兰卫生部2016/17年度数据探索报告,目前吸烟的人群为:
在2016/17年度,目前的吸烟者人数有所下降,从2006/07年度的20.1%下降到约60万(15.7%)名成年吸烟者
毛利成人目前的吸烟者从2006/07年的42%下降了35%
目前有24%的太平洋成年吸烟者与上次调查相比没有明显下降。
35岁及以上的成年人降低了年轻人的吸烟率,但没有明显下降。
社会经济因素是成年人当前吸烟习惯的共同决定因素。研究发现,社会经济贫困地区的大多数成年人是目前吸烟者的三倍。
Tairawhiti吸烟率流行
泰拉希提岛(Tarawhiti)的吸烟历史已有数十年之久。多年来,已经做出了许多努力来减少该地区的烟草使用者的数量。我们将探索,他们的努力是有效的。
在2006-2007年的新西兰健康调查中,可以确定,塔拉威蒂烟民是所有地区卫生委员会中吸烟人数最多的。在塔拉威提居民中,超过30%是吸烟者,是该地区吸烟率最高的群体。在塔拉威蒂,每年使用烟草造成70例死亡,其中毛利人死亡更多。
以下统计数据是根据新西兰2013年有关塔拉希提地区吸烟率的人口普查统计数据得出的。
抽烟
图2:14–15岁从未吸烟的学生比例的趋势,按性别,TairāwhitiDHB,1999–2013
资料来源:ASH 2013年第十年快照调查
从图中可以看出,在过去的十五年中,Tairawhiti的吸烟者人数显着增加。 2013年,有49%的人从未吸烟。
图3:15-17岁,18-19岁,20-24岁的常规吸烟者,塔伊拉赫蒂(Tairāwhiti)DHB,2013年
资料来源:2013年人口普查,新西兰统计局
注意:普通吸烟者每天要抽一根或多支香烟。
从图中可以看出,自2006年以来,Tarawhiti的年轻人中吸烟率显着下降。但是,在18-24岁的年轻人中,成年后吸烟率更高。 2013年,年龄在20-14岁之间的毛利人中有49%经常吸烟。另一方面,每组中非毛利人定期吸烟的可能性是毛利人的一半。
吸烟状况
表38:15岁及15岁以上的吸烟状况,泰拉惠蒂DHB,2006年和2013年
| Smoking status | Māori | Non-Māori | Māori/non-Māori
ratio (95% CI) |
Difference in proportion | ||||||||
| Number | % | (95% CI) | Number | % | (95% CI) | |||||||
| 2006 | ||||||||||||
| Regular smoker | 5,265 | 45.2 | (44.3, | 46.1) | 3,363 | 23.3 | (22.5, | 24.1) | 1.94 | (1.87, | 2.02) | 21.9 |
| Ex-smoker | 2,256 | 17.0 | (16.4, | 17.7) | 4,242 | 19.4 | (18.7, | 20.1) | 0.88 | (0.83, | 0.92) | -2.4 |
| Never smoked | 4,554 | 37.7 | (36.8, | 38.6) | 9,414 | 57.2 | (56.3, | 58.1) | 0.66 | (0.64, | 0.68) | -19.5 |
| 2013 | ||||||||||||
| Regular smoker | 4,482 | 38.4 | (37.5, | 39.3) | 2,373 | 16.5 | (15.8, | 17.2) | 2.33 | (2.22, | 2.45) | 21.9 |
| Ex-smoker | 2,832 | 19.7 | (19.0, | 20.4) | 4,344 | 19.7 | (19.1, | 20.4) | 1.00 | (0.95, | 1.05) | 0.0 |
| Never smoked | 5,127 | 41.9 | (41.0, | 42.8) | 9,711 | 63.6 | (62.7, | 64.5) | 0.66 | (0.64, | 0.68) | -21.7 |
资料来源:新西兰统计局2006年和2013年人口普查
注意:%是2001年毛利人的年龄标准化
普通吸烟者每天要抽一根或多支香烟。
统计数据显示,2006年至2013年期间,毛利人的成人定期吸烟者比例从45%大幅下降至38%。毛利人不吸烟者和前吸烟者的比例有所增加。但是,2013年在塔拉希提岛,毛利人和非毛利人之间的吸烟率之间存在22%的差异。
根据新西兰卫生部2014-2017年刊《年度数据浏览器》,吸烟者目前的状况使Tairawhiti成为新西兰烟草使用的领先者。
非法用药-安非他明 健康问题代写
根据针对整个新西兰的《 2014/15年苯丙胺使用情况:新西兰健康调查》,过去一年中有0.9%的成年人使用苯丙胺。这相当于新西兰人口的26,000。过去一年该药的平均使用年限为33年,而2012/13年为29年。
在过去的一年中,年龄在25-34岁之间的年轻人更普遍使用苯丙胺,其次是16-24岁的年轻人。苯丙胺的最低使用者是55-64岁。
但是,自2012-13年以来,过去16至24岁的苯丙胺使用者的流行率一直呈下降趋势。统计数据还显示,去年男性中的苯丙胺使用量为1.2%,高于女性的0.7%。
该调查还确定,毛利人使用苯丙胺的患病率高于毛利人。在过去的一年中,毛利人中有1.6%,亚洲人中有0.1%,太平洋人中有0.2%,欧洲人中有1.1%使用了苯丙胺。在过去的一年中,发现毛利人使用苯丙胺的流行率是非毛利人的1.8倍。
表1:新西兰过去16至64岁成年人过去一年的苯丙胺使用情况
| Year | Survey | Mode | Prevalence |
| 2003 | Health Behaviours Survey – Drug Use | Telephone interview | 2.7% (2.3–3.3) |
| 2007/08 | New Zealand Alcohol and Drug Use Survey | Self-completed interview | 2.2% (1.7–2.7) |
| 2011/12 | New Zealand Health Survey | Face-to-face interview | 0.9% (0.7–1.1) |
| 2012/13 | New Zealand Health Survey | Face-to-face interview | 0.9% (0.7–1.2) |
| 2013/14 | New Zealand Health Survey | Face-to-face interview | 1.1% (0.8–1.4) |
| 2014/15 | New Zealand Health Survey | Face-to-face interview | 0.9% (0.7–1.1) |
资料来源:卫生部,2007年;卫生部,2009年; NZHS 2011 / 12、2012 / 13、2013 / 14和2014/15的数据
塔拉希提岛的苯丙胺使用
根据2014-2017年《年度数据资源管理器》,泰拉希提的苯丙胺使用率为0.8%(CI 0.2-2.0)。数据显示,对于15岁及以上的成年人,苯丙胺的使用量从2011-14年的0.5%(CI 0.1-1.5)显着增加到2014-17年的0.8%(CI 0.2-2.0)。
15至24岁的年轻人使用苯丙胺的患病率最高,为2%(CI 0.1-9.4)。 45-64岁的人群使用苯丙胺的可能性最低,为0.2%(CI 0.0-1.1)
通常,年龄在15-24岁之间的男性患病率比同年龄组的女性高3.6%(CI 0.1-20.0),患病率为0.6%(CI 0.0-6.3)。毛利妇女使用安非他明的比例为1.2%(0.4-3.0),而男性为0.4%(CI 0.0-2.7)。
这些图表提供了指定人口中的患病率(即受影响人口的百分比)
资料来源:2014-17年年度数据浏览器
体育锻炼
新西兰每年在卫生上的花费超过132亿美元,占年度总支出的19%(卫生部2011a)。因此,对于新西兰政府而言,促进其人口的预防性医疗保健以确保可持续的医疗保健体系变得至关重要。
体育锻炼是预防性保健活动的一部分。定期运动会降低患心血管疾病和全身健康护理的风险。每天进行30分钟的体育锻炼对于改善健康至关重要。
体育锻炼对健康具有以下重要性:
改善胆固醇水平
降低血压
帮助减肥并保持健康的体重
控制血糖(糖)水平
帮助您改善睡眠质量,减轻压力
在塔拉希提岛很少或根本没有体育锻炼
通常,与塔拉威提人群中的任何其他年龄组相比,很少或不进行体育锻炼的65岁及以上人群的患病率更高(38.1%(CI 29.8-47.2))。 15岁及以上所有年龄段的女性比同年龄段的男性进行很少或几乎没有体育锻炼的患病率更高。毛利族妇女由于缺乏体育锻炼而患病率最高,为38.2%(CI 30.9-46.0)。
这些图表提供了指定人口中的患病率(即受影响人口的百分比)
资料来源:2014-17年年度数据浏览器
身体大小
在此子主题下,本报告将探讨新西兰肥胖流行病的现状。它将讨论在不同年龄段受肥胖影响最大的人群亚组。它还将查看人口集中最普遍的个体群体。
超重是多种疾病的风险因素之一,包括心脏病,中风,2型糖尿病和其他类型的癌症。肥胖还会增加不孕,肌肉骨骼问题,睡眠呼吸暂停和痛风的风险(WHO 2000)。根据卫生部(2013a)的数据,高体重指数(BMI)是导致新西兰疾病和残疾的三大风险因素之一。肥胖人群的预期寿命缩短了约8-9年(Whitlock等,2009)。
经合组织(2014年)指出,过去几十年来,全球肥胖症患病率急剧上升。在新西兰,肥胖和超重已影响了三分之二以上的成年人口和三分之一的儿童。成人肥胖症的患病率增加了三倍,从1977年的10%到2011-13年间的30%在新西兰。
Swinburn(2008)解释了肥胖增加的原因,这在很大程度上归因于现代生活方式和生活环境。
在过去的三十年中,人们目睹了体育锻炼的减少以及廉价,高能量和营养不良的食品的出现。这份报告着眼于肥胖流行如何影响了塔拉希提岛不同的出生人群。
以下是新西兰肥胖统计数据的摘要。从该图可以看出,在2011年至2013年之间,新西兰35%的成年人超重,而30%的肥胖。男性中超重的患病率高达39%,而女性中这一比例为30%。而且,肥胖随着年龄的增长达到最佳,年龄在65-74岁。
图1:2011-2013年各个BMI类别中成年人的比例
图2:2011-2013年按性别和种族划分的肥胖率和极端肥胖率
Tairawhiti的超重和肥胖症 健康问题代写
根据《 2014-17年度数据浏览器》,塔拉希提岛以超重和肥胖症的患病率为71.8%(CI 66.6-76.6),排名第四。从2011-2014年的超重和肥胖症患病率增加了,Tarawhiti的2014-2017年患病率为71.8%(CI 66.6-76.6)。
平均而言,在45岁以上的人群中,超重和肥胖的患病率较高。患病率随着年龄在45岁及以上的年龄而增加,是最缺乏的患病率超过72%。男性超重和肥胖的患病率高于女性,平均患病率超过82%。
这些图表提供了指定人口中的患病率(即受影响人口的百分比)
资料来源:2014-17年年度数据浏览器
在当今世界,健康的人口一直是政府和整个社会的首要任务。需要解决影响人民福祉的健康问题,并实施可持续的解决方案。新西兰受到各种风险因素的影响,这些风险因素在不同年龄段的人群中导致大量健康问题。另一方面,塔拉维希提地区的健康问题表明该国人口高度匮乏。新西兰社区和政府都做出了许多努力,以使人口摆脱这些风险因素的影响。
References 健康问题代写
Annual Data Explorer. (2017, May 10). Regional Results 2014-2017: New Zealand Health Survey. Retrieved from https://www.health.govt.nz/publication/regional-results-2014-2017-new-zealand-health-survey
OECD. 2014. OECD Obesity Update 2014. Paris.
ASH Year 10 Snapshot. (2013). ASH Year 10 Snapshot smoking survey. Retrieved from https://www.hpa.org.nz/sites/default/files/documents/NZYTM%20information%20for%20people%20working%20with%20schools-FINAL.pdf
New Zealand Census. (2013, March 5). Census | Stats NZ. Retrieved from https://www.stats.govt.nz/topics/census
Ministry of Health. 2013a. Health Loss in New Zealand: A report from the New Zealand Burden of Diseases, Injuries and Risk Factors, 2006–16. Wellington: Ministry of Health.
Whitlock G, Lewington S, Sherliker P, et al. 2009. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet 373(9669): 1083–96.
Swinburn B. 2008. Obesity prevention: the role of policies, laws, and regulations. Australia and New Zealand Health Policy 5(1): 12.
Ministry of Health. 2007. Drug Use in New Zealand: Analysis of the 2003 New Zealand Health Behaviours Survey – Drug Use. Wellington: Ministry of Health.
WHO. 2000. Obesity: Preventing and managing the global epidemic. Report of a WHO Consultation (WHO Technical Report Series 894).
Hauora. (n.d.). Tairawhiti – region » Tairawhiti District Health. Retrieved from http://www.tdh.org.nz/about-us/tairawhiti-our-region/
附录


